7b - Surveillance of severe acute respiratory infections associated with SARS-CoV-2, influenza virus and RSV using ICD-10 codes: a case definition accuracy study across five European countries, 2021-2023
Poster tour posters
Information
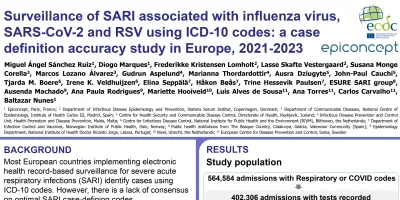
Background : Surveillance of severe acute respiratory infections (SARI) using ICD-10 codes from electronic health records (EHR) lacks consensus on the optimal SARI case-defining codes. We aimed to identify codes that maximise the sensitivity (Se) and positive predictive value (PPV) for the surveillance of SARI associated with SARS-CoV-2, influenza, and respiratory syncytial virus (RSV) in Denmark, Iceland, Malta, Norway, and Spain.
Methods : We included hospitalisations in weeks 21/2021 to 39/2023, with first-three-character respiratory disease or four-character COVID-19 ICD-10 codes; and SARS-CoV-2, influenza virus or RSV tests. We assessed the Se and PPV of individual codes against laboratory confirmation and calculated the combined Se/PPV rank-sum. For each pathogen, we incrementally combined up to 10 codes based on their rank-sum, to identify code sets that maximised the Screening-Marker Index (SMI= Se*PPV): excellent (>=0.81), good (>=0.64), satisfactory (>=0.49), and poor (<0.49) utility.
Results : We included 401,215 hospitalisations. For laboratory-confirmed SARS-CoV-2; code U07.1 (B34, B97 for Denmark) yielded excellent utility in Denmark, Malta, Norway and Spain (Se>=0.88, PPV>=0.90, SMI>=0.82) and good utility in Iceland (Se: 0.97, PPV: 0.81, SMI:0.79). For influenza virus; the utility of J09, J10, J11 was excellent in Denmark, Spain and Norway (Se>=0.84, PPV>=0.97, SMI>=0.83), satisfactory in Malta (Se: 0.56, PPV: 0.93, SMI: 0.52), and poor in Iceland (Se: 0.72, PPV: 0.60, SMI:0.43). For RSV, key codes included J12, J20, J21 and J96, but utility was poor (Se: 0.35-0.91, PPV: 0.25-0.71, SMI: 0.17-0.34).
Conclusions Our findings recommend using codes U07.1, J09-J11 for identifying SARS-CoV-2 and influenza-associated SARI, and assessing the accuracy of four-character codes for RSV (e.g., J12.1). The applicability of our results may depend on surveillance systems’ characteristics, coding practices, and the epidemiology of SARI. Therefore, context-specific assessments are recommended.